
What an ideal MBBS exam should look like
Do you remember the time you were in primary school? We had awesome recesses back then. Half of it went into eating and prattling, and the rest we would spend gamboling around. Those were the days we actually had some zest and order in our lives: waking up early in the morning with excitement for school (which would bump it’s head hard once we reached there!); the exhilaration of having tied our shoe laces on our own; the frolic and frisk in the evening that would rejuvenate our mind like nothing else; and then, between 8-10 in the night, witness the most productive study hours of all time.
But there is something that would seem much unwelcoming as your mind recaps those days. Those were the times when we started embracing the ‘Read and write’ or ‘theory’ culture that extends much into our undergraduate study today. Answers, essays, poems and ‘fill in the blanks’ were meant to be mugged up. Swotters even ended up with vivacious pictures of texts and paragraphs in their minds. It’s a legacy that we’ve carried with ourselves all along, and the picture in MBBS can be no different. The fact that a lot of MBBS revolves around theory at the expense of practicals doesn’t need an explanation. To chew on it is a topic for another day. What I intend to bring out through this write-up is a tangible facet of our system of theory examinations that goes beyond our ‘Read and write’ attitude and fortifies the theory favoritism MBBS exhibits today.
To Categorise Learning
Before we set foot into the prime domain of our discussion, it would be better if we brush up the way we bracket what we learn. I hope this flowchart would serve this purpose since it sits quite well with me:
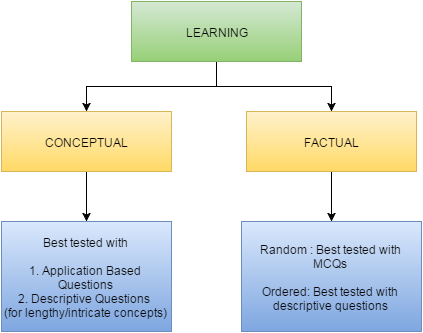
As you can see, I’ve classified learned information into concepts (those involving a train of logic) and facts (those that need to be remembered). The facts are further classified as random( discrete) and those with a specific order( a collection of related facts). I am very well aware that these distinct categories will seem to merge into one if we look into the depths, but I have no problem allowing them to be distinct for most practical purposes.
The Current Picture
Now, we are all familiar with how a theory examination paper looks like. The following is how I would put it down empirically:
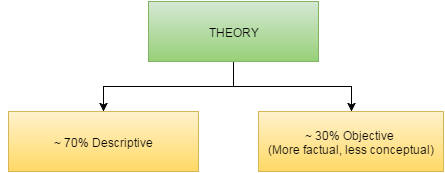
It’s notable that a large part of it is centered around descriptive questions( where you have to write on something at length). What’s even more obvious is the feeble proportion of what I call ‘application based’ or ‘concept-testing’ questions. An application based question tests the perfection with which one can apply core concepts in practical settings, unlike a descriptive question that demands to put down and explain the concept itself. You can relate it to many of those that you come across in USMLE exams. Take the following as an example:
“A 24-year-old woman presents to the emergency department with severe diarrhoea. When she is supine, her blood pressure is 90/60 mm Hg ( decreased) and her heart rate is 100 beats/min (increased). When she is moved to a standing position, her heart rate further increases to 120 beats/min. What accounts for the further increase in heart rate after standing?”
-Taken from BRS Physiology 6th edition.
As evident and obvious on the slightest focused thinking, an application based question takes conceptual assessment a step further from a descriptive question, since to be able to actually apply learned concepts is a skill much more desirable and serviceable than plainly putting them down in raw form. Further, the ability to successfully apply a concept is a stronger proof of the force and clarity it sits in the mind with- besides being closer to real life and harder to be escaped from than writing a descriptive answer.
The Body of the Problem
As much as it’s evident from the foregoing discussion- that our theory exams are relatively ineffective when it comes to testing core conceptual understanding, the problem stretches much beyond it.
A close look at a descriptive answer will reveal that it often doesn’t pertain to a single category: either concepts, random or ordered facts- and that many descriptive answers are a mixture of these in varied proportions. Also, you always need to work a bit here and there, cram a few lines, adjust the size of your answer and work a lot on your presentation- most of which is relatively impertinent as far as the final goal of learning medicine is concerned. A descriptive answer meant to explain a concept is more than a simple presentation of the concept but a distinct ‘set’ of information that has to be sculpted precisely and methodically.
What if such sets are spread across the MBBS syllabus? You can see the already hefty theory curriculum turn more cumbersome and time-consuming. In the presence of theory favoristism, this is going to come at the expense of practical learning. This is exactly what happens today. Theory’s superiority is emboldened by this feature which is deeply ingrained in our examinations.
Moreover, learning becomes more source-centric than knowledge-centric. Few students ever turn to articles, journals and other medical literature. The textbook becomes the virtual bible. Last but not the least, descriptive questions allow more room for practices like cramming than application based questions.
Envisioning the Solution
Don’t mistake me as a partisan against descriptive questions. Descriptive questions have their own place and importance. They are possibly the best we can put into use for assessing lengthy and intricate concepts. Also, I see little of any other credible way to test factual (ordered) questions. What we need to understand is that we are being grossly imprudent while confining conceptual assessment to written treatises and paragraphs. By evading the topic of application based questions, we will only be missing out on something that can deliver so much to our betterment.
We need to scale up the proportion of application based questions in our theory exams. A good way to kick it off is to introduce application based MCQs, and then gradually put it into the mould of short answers. Descriptive questions can be reserved for the purposes mentioned above. Something like a 60:40 ratio would do perfectly fine.
I can fore see how much this rational change in the way we design our theory exams can do to revitalise medical education in more than one way. Besides a more efficient and coherent manner of testing concepts, the gargantuan MBBS syllabus can be covered with much more uniformity, and in much lesser time. Stress on rather superfluous and impertinent areas like writing skills can be safely removed. Malpractices and cramming can be circumvented, understanding can be fostered and a healthy equilibrium can be struck between practicals and theory.
The ‘Read and write’ attitude is something that gets rooted into our minds far early in our academic expedition. It stretches right from primary school, and to talk of it in terms of MBBS alone is deficient. What makes me highlight this theory favoritism with respect to MBBS is that it’s more of an applied sphere than anything I can possibly imagine. The need here, for change to be born, is like in any other: we need to rise from the slumbers of our self- imposed dogmas, and I wish this write-up would be a nudge towards that purpose.
About the Author

Dr. Soham Bhaduri is an avid-thinker on medico-social issues and a blogger at ‘Free Thinking Medic’
(Disclaimer: The views and opinions expressed in this article are those of the author and do not necessarily reflect the views of Daily Rounds)
Image Credits: http://www.sriramachandra.edu.in/